
Extreme blood sugar highs and lows can lead to major problems:
- Hypoglycemia (low blood sugar) can happen quickly and is important to treat right away. It can cause confusion and disorientation, or be more severe and cause loss of consciousness, seizure or coma.57, 58
Fear of hypoglycemia is when some people living with diabetes keep their blood glucose high to avoid severe hypoglycemia. This may lead them to make poor diabetes-management decisions, which can be a barrier to achieving their target glucose levels and lead to increased risk of diabetes complications.59
Hypoglycemia unawareness (or impaired hypoglycemia awareness) is when a person with diabetes doesn’t notice they have low blood sugar, as they do not experience usual early warning symptoms. Without warning, they lapse into severe hypoglycemia and may become confused or disoriented, experience convulsions or, in rare cases, fall into a coma.60, 61
- Hyperglycemia (high blood sugar) can cause long-term health complications caused by damage to blood vessels and nerves such as heart disease, kidney failure, stroke, heart attack, blindness and lower limb amputation as well as diabetic ketoacidosis, which is a poten-tially life-threating buildup of acids in the blood.62, 63
i. Monitoring Glucose Levels
There are a variety of ways to monitor glucose levels64, 65, 66
Capillary blood glucose meter (formerly known as blood glucose meter) uses a finger prick to check blood glucose levels.67
Intermittently scanned continuous glucose monitoring (isCGM) (formerly known as flash glucose monitoring) measures interstitial fluid glucose levels* with a hand-held scanner swiped over the sensor. Some systems are equipped with optional alarms to alert for low and high blood sugar.
Real-time continuous glucose monitoring (rtCGM) (formerly known as continuous glucose monitoring or CGM) also checks interstitial fluid glucose levels*; however, it provides a continuous display of blood sugar and uses an alarm to alert for low and high blood sugar.
A1C, also known as HbA1c, is a laboratory blood test that measures average blood sugar over the past three months.
*Works via a small sensor that is inserted just under skin that reads the glucose level in the surrounding interstitial fluid, which is a thin layer of fluid that surrounds the body’s cells.
ii. Time in Range70, 71, 72, 73, 74, 75
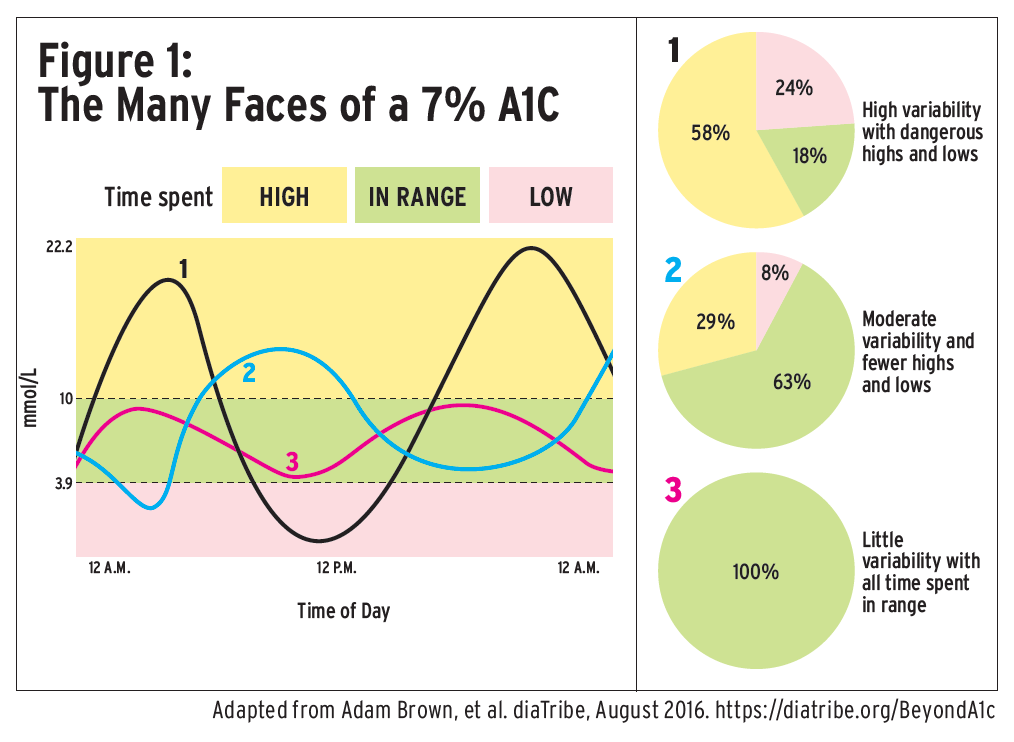
Instead of measuring average blood sugar via the A1C test, there is growing interest from diabetes experts in tracking time in range (TIR): the percentage of time that a person’s blood glucose level is in their recommended target range (see Glucose Targets). The A1C average does not capture glycemic variability, the fluctuations in glucose values of people living with diabetes. Two people can have the same A1C value but have a wide range of high and low blood glucose values, which results in a different TIR (see Figure 1).
A mean speed of 80 km/h over the past three months of commuting will never reflect times when a vehicle is racing at 150 km/h and far in excess of the speed limit or is slowed to 15 km/h in traffic congestion. Similarly, the clinician receives only the most basic of information from the HbA1c measurement and masks the occurrence and frequency of dangerous highs and lows.76
Time in range goals may be individualized for each person; however, generally people with diabetes should aim to be in-range as much as possible, with a recommendation of least 70% TIR. Evidence is growing that increased TIR reduces the likelihood of diabetes complications. Experts indicate that a TIR of 70% equates to an A1C of about 7%, and each 10% increase in TIR equates to a 0.5% decrease in A1C.
iii. Evidence-Based Guidance for Blood Glucose Monitoring
Diabetes Canada recently updated its blood glucose monitoring recommendations77, 78 for Canadians living with diabetes to reflect new and emerging research that has been conducted within the past few years. The recommendations on glucose monitoring type and frequency prioritize safety and improved outcomes for people living with diabetes. These recommendations offer healthcare providers evidence-based guidance on the types of devices that are best suited to people living with diabetes based on their disease type, medications and treatment goals.
Benefit plan managers may find it helpful to refer to these recommendations to determine coverage of glucose monitoring devices for employees or their family members living with diabetes.
iv. Benefits of Glucose Monitoring Devices79, 80, 81, 82, 83, 84, 85
According to Diabetes Canada, glucose monitoring devices such as intermittently scanned continuous glucose monitoring (isCGM) (formerly known as flash glucose monitoring) and real-time continuous glucose monitoring (rtCGM) (also known as continuous glucose monitoring or CGM) “have the potential to improve blood sugar management and quality of life for people living with diabetes, resulting in physical, social, emotional, and functional benefits.”86
Glucose monitoring technologies allow the person with diabetes to collect more data about their glucose, says Tanner, and “drive behaviour and lifestyle changes to improve their condition and make the day-to-day life with diabetes easier.”
Not only do the devices eliminate many of the finger pricks required by more traditional glucose
meters, but they also help people with diabetes stay within their target blood sugar range. Traditional blood glucose monitoring and A1C tests don’t capture glucose variability (the ups and downs of sugar levels) and don’t provide any indication of trends.
The devices may have alarms that alert people or their caregivers when their levels drop too low, for example, overnight while sleeping or while a child with diabetes is at school.
This can be particularly helpful for people with hypoglycemia unawareness.
Glucose monitoring devices can track and report glucose historical trend information, which allows the person with diabetes and their healthcare team to analyze glucose patterns and adapt treatment as needed. The devices allow remote tracking by healthcare providers to support digital diabetes care. In addition, real-time continuous glucose monitoring (rtCGM) can be integrated with insulin pumps to develop hybrid closed-loop insulin delivery systems (HCL), which automatically adjust insulin delivery based on rtCGM input.
Small Reduction Offers Significant Benefits
Reducing a person’s A1C by as little as 1% can lead to significant short and long-term clinical benefits.
Interventions or programs that reduce a person’s A1C by as little as 1% can lead to significant short- and long-term clinical benefits, including a 37% reduction in microvascular complications,87 43% reduction in amputations, 14% reduction in heart attacks and 12% reduction in strokes, and up to 21% reduction in deaths related to diabetes.88
v. Insulin Treatment89
Insulin therapy is required for the management of type 1 diabetes and sometimes type 2 diabetes. It is prescribed by healthcare providers based on people’s goals, lifestyle, meal plan, age and general health, as well as social and financial factors.
Insulin is injected by pen, syringe or insulin pump, and healthcare providers work with people with diabetes to determine the number, timing and dose of daily injections needed per day and whether an insulin pump is appropriate. The objective is to achieve blood glucose levels that are as close to target as possible to decrease hyperglycemia and avoid hypoglycemia.
v. Insulin Pumps90, 91,92,93
Insulin pumps94 are an alternative to multiple daily insulin injections, and their clinical effectiveness is well documented. Diabetes Canada’s Clinical Practice Guidelines state that insulin pump therapy can be beneficial for some people with type 1 diabetes.
Pumps can closely mimic the normal action of a healthy pancreas and allow glucose levels to be managed more precisely. They can be programmed to increase or decrease the amount of insulin delivered for a specified period or can calculate recommended insulin correction doses.
Insulin pumps can be life-changing for individuals living with type 1 diabetes, says Tanner. “Imagine having diabetes from a very young age, needing insulin injections four or more times per day. In one year alone, you would need a least 1,460 injections. An insulin pump takes away some of this burden.”
An insulin pump also allows flexibility with insulin delivery, explains Tanner. “A person can adjust their insulin depending on what they are doing and what they are eating, allowing them to match their insulin more precisely to their individual needs.”
Evidence shows that insulin pump users can achieve lower blood sugar levels, more time in range, less risk of hyperglycemia and hypoglycemia, and fewer associated long-term diabetes complications.
vii. Type 2 Diabetes Glucose-Lowering Medications95
As a complement to healthy behaviour interventions and lifestyle modifications, there are a variety of medications that may be used to treat type 2 diabetes that can help people achieve their target blood glucose levels. Diabetes Canada provides medication recommendations and encourages healthcare providers to work together with their patients to determine which medication(s) can help them achieve their best health.
|
First-line medication |
|
|
Metformin |
Makes the body respond better to insulin anduse it more effectively. Reduces liver’sglucose production. |
|
If metformin and healthy behaviour changes are not enough to manage blood glucose levels, second-line medications can be added. |
|
|
Second-line medications |
|
|
DPP-4 inhibitors |
Lower blood glucose by increasing insulin levels after meals and lowering glucagon levels (a hormone that raises blood glucose). |
|
GLP-1 receptor agonists |
Act when blood glucose increases after eating. Increase insulin levels, which helps lower blood glucose and lower glucagon levels (a hormone that raises blood glucose). |
|
SGLT2 inhibitors |
Eliminate glucose into the urine. |
|
Insulin secretagogues (meglitinides, sulfonylureas) |
Help the pancreas release more insulin. |
|
Thiazolidinediones |
Make the bodys tissues more sensitive to insulin. |
|
Insulin therapy |
Some people with type 2 diabetes need insulin therapy as well. Healthcare provider prescribe based on individual needs. |

